
Laser therapy may offer fast-acting option for CSR resolution
Patients tolerate therapy well; high safety profile allows re-treatment as necessary




Central serous retinopathy (CSR) is distinguished by a vascular focal leakage occurring through the retinal pigment epithelium (RPE), which results in serous detachment of the neurosensory retina.
This condition may be instigated or exacerbated by corticosteroid use or stress. This disease is typically self-healing within a few months, and while patients are generally left with good visual acuity, chronic CSR may develop in 33%-50% of cases which can lead to other issues such as progressive RPE atrophy and permanent visual impairment.
Discontinuing corticosteroid use will aid in disease resolution, however, postponing more effective and immediate treatment may intensify patient stress levels, further aggravating the disease
Treatment options
Aside from waiting for the disease to self-resolve, treatment options typically include oral and topical medications, photodynamic therapy (PDT), laser photocoagulation, and antiVEGF injections. Some physicians advocate the use of bevacizumab (Avastin, Genentech) injections, however this use is off label and I have found no evidence of any beneficial use. Spirinolactone, an aldosterone antagonist, can be effective though it may result in gynecomastria, a side effect that most men will not tolerate.
PDT and conventional, continuous-wave laser photocoagulation have been successful but are not ideal as they may result in negative side effects. PDT can cause photosensitivity and choroidal hypoperfusion while continuous-wave laser photocoagulation can cause central or paracentral scotomas, contrast sensitivity loss, foveal damage, retinal distortion, and thermal damage to photoreceptors.
Laser therapy
Laser therapy technology chops a continuouswave laser beam into short on and off pulses which enables the clinical to finely regulate and maintain temperature rise at the target tissue without causing lethal damage to the RPE or surrounding tissue.
Laser therapy (MicroPulse laser therapy) triggers an anti-angiogenic and restorative biological response resulting in the re-absorption of sub retinal fluid through the restoration of the RPE cells. With no lethal damage to the
RPE or retina I can confidently provide a safe treatment with significant beneficial effects. I have found utilizing the laser treatment mode of the IQ 577 yellow laser (IRIDEX) to be the best option for my acute and chronic CSR patients as laser therapy is highly beneficial without the safety concerns of continuous-wave laser treatment.
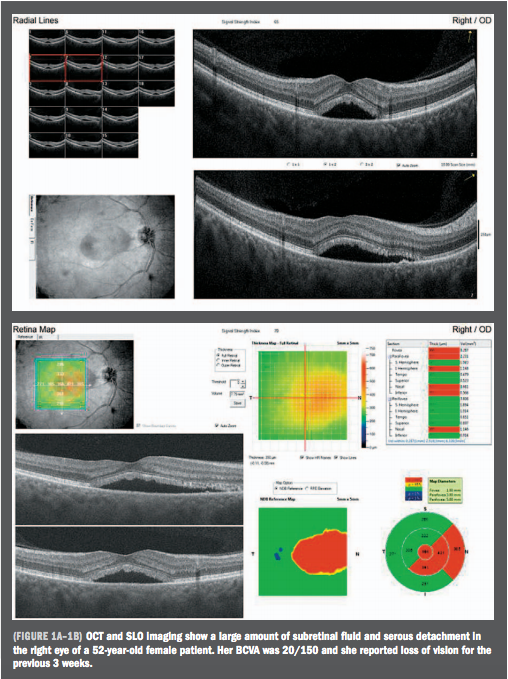
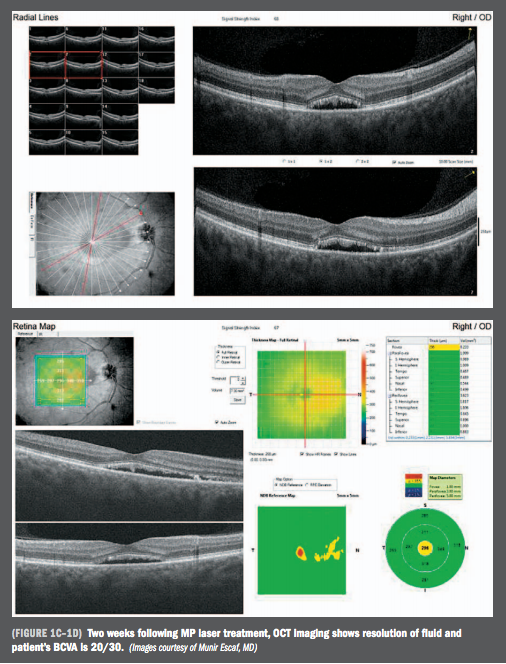
As an example, I performed laser therapy on a 52-year-old female patient with CSR a substantial amount of subretinal fluid in her right eye that had caused loss of vision for three weeks. Two weeks following treatment, the fluid was resolved and her vision had improved from 20/150 to 20/30.
Treatment with continuous-wave laser can cause tissue damage resulting in central visual field loss, loss of contrast sensitivity, and other visual issues if it is delivered too near the foveal area. Having an effective treatment option that creates immediate improvement without the risks associated with conventional laser greatly eases patients’ minds.
Patient treatment results
I compared a control group of my CSR patients that I observed, and a treatment group of patients who received laser therapy. Prior to treatment mean best-corrected visual acuity (BCVA) of all patients was 20/50. Four weeks after treatment, mean BCVA in the control group improved to 20/32 and mean BCVA in the treated group improved to 20/25. In addition, approximately 25% of patients in the control group had resolution of subretinal fluid, compared to more than 80% of the treatment group.
While CSR may eventually resolve with no treatment, waiting for the symptoms to improve can increase the anxiety of already overly stressed patients and put them at risk for a chronic condition. The laser therapy offers patients a fast-acting option for a resolution in a clinical disease that typically requires us to wait of two to four months and hope for resolution.
Additionally, patients tolerate laser therapy very well as there is no discomfort, and its high safety profile allows retreatment as often as necessary. The ability to provide my patients with this quick, painless, and effective treatment is invaluable.
Disclosures:
Munir Escaf, MD
E: munirescaf@hotmail.com
Dr. Escaf is an ophthalmologist and surgeon at the Centro Oftalmologico Carriazo in Barranquilla, Colombia. He did not indicate any proprietary interest in the subject matter.
References:
1. Agarwal A, Garg M, Dixit N, Godara R. Evaluation and correlation of stress scores with blood pressure, endogenous cortisol levels, and homocysteine levels in patients with central serous chorioretinopathy and comparison with age-matched controls. Indian Journal of Ophthalmology. 2016;64:803-805. doi:10.4103/0301-4738.195591.
2. Gilbert CM, Owens SL, Smith PD, Fine SL. Long-term follow-up of central serous chorioretinopathy. Br J Ophthalmol. 1984;68:815-820.
3. Loo RH, Scott IU, Flynn Jr, HW, Gass JD, Murray TG, Lewis ML et al. Factors associated with reduced visual acuity during long-term follow-up of patients with idiopathic central serous chorioretinopathy. Retina.2002;22:19-24.
4. Bujarborua D. Long-term follow-up of idiopathic central serous chorioretinopathy without laser. Acta Ophthalmol Scand. 2001;79:417-421.
5. Piccolino FC, Eandi CM, Ventre L, et al. Photodynamic therapy for chronic central serous chorioretinopathy. Retina. 2003;23:752-763.
6. Khosla PK, Rana SS, Tewari HK, Azad RU, Talwar D. Evaluation of visual function following argon laser photocoagulation in central serous retinopathy. Ophthalmic Surg Lasers. 1997;28:693-697.
7. Maruko I, Iida T, Sugano Y, Ojima A, Ogasawara M, Spaide RF. Subfoveal choroidal thickness after treatment of central serous chorioretinopathy. Ophthalmology. 2010;117:1792-1799.
8. Fudemberg, SJ, Myers, JS, Katz, LJ, et al. Trabecular meshwork tissue examination with scanning electron microscopy: a comparison of MicroPulse diode laser (MLT), selective laser (SLT), and argon laser (ALT) trabeculoplasty in human cadaver tissue. Invest Ophthalmol Vis Sci. 2008;49:1236.
9. Ogata N, Tombran-Tink J, Jo N, et al. Up regulation of pigment epithelium-derived factor after laser photocoagulation. Am J Ophthalmol. 2001;132: 427-429.
Newsletter
Keep your retina practice on the forefront—subscribe for expert analysis and emerging trends in retinal disease management.











