Determining the time to DME resolution with intravitreal aflibercept
Speaking at the American Society of Retina Specialists 2021 annual meeting in San Antonio, Rishi P. Singh, MD, provided results of the VISTA and VIVID studies, and he pointed out that the findings could help physicians set expectations of DME therapy.


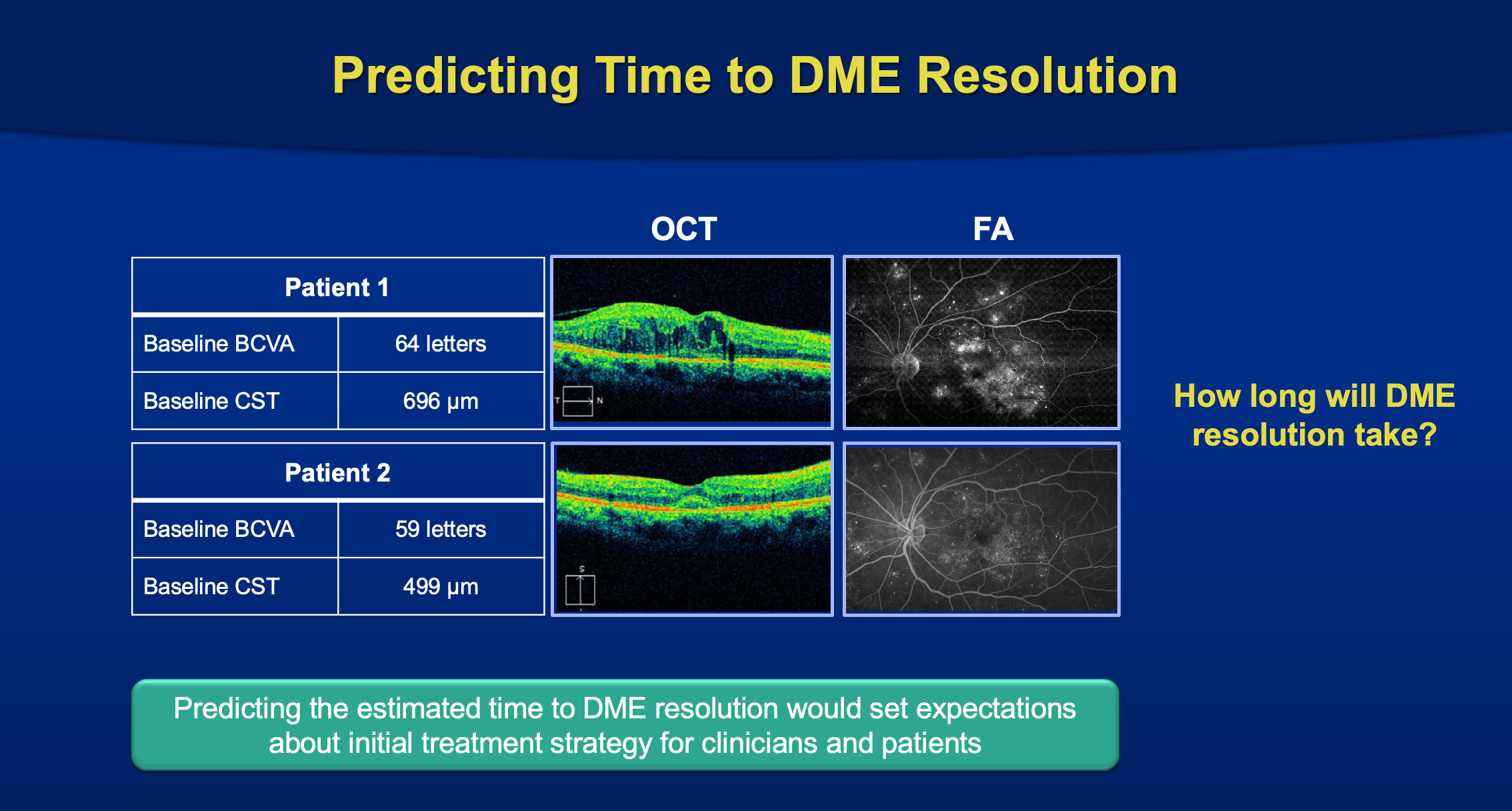
The pooled data from the VISTA and VIVID clinical trials on the use of intravitreal aflibercept injections (IAI) (Eylea, Regeneron Pharmaceuticals) to treat diabetic macular edema (DME) identified thicker central subfield thickness (CST) and better best-corrected visual acuity (BCVA) as baseline factors associated with a longer time to and lower rate of resolution of DME.
Rishi P. Singh, MD, Carolina Valentim MD, and Katherine Talcott, MD, reported the study results at the American Society of Retina Specialists 2021 annual meeting in San Antonio, Texas, on behalf of the VISTA and VIVID study investigators. The coauthors are from the Center for Ophthalmic Bioinformatics at the Cole Eye Institute, Cleveland Clinic, in Cleveland., Ohio
A step beyond VISTA and VIVID
These studies were multicenter, double-masked trials that included patients with clinically significant DME with central macular involvement and BCVAs ranging from 20/40 to 20/320. Patients were randomly assigned to 1 of 2 dosing intervals of the study treatment or laser.
The results showed that IAI significantly improved the visual and anatomic outcomes compared with laser after 52 weeks, and these results were maintained out to 100 weeks.
As with any disease, one of the first questions always concerns its resolution.


Rishi P. Singh, MD
“Predicting the estimated time to DME resolution would set expectations about the initial treatment strategy for clinicians and patients,” Singh said. “Since the clinical responses to DME treatment may vary, identifying baseline factors associated with the time to DME resolution may help set expectations for clinicians and patients during the initial treatment period.
To identify these factors, Singh and his colleague looked at how the baseline patient characteristics affected the time to DME resolution in patients treated with IAI or laser in the 2 trials.
The investigators combined the demographic, systemic, and ocular characteristic data from the VISTA/VIVID patients treated with IAI, which included age, sex, race, ethnicity, diabetes type and duration, hemoglobin A1c, hypertension, hyperlipidemia, and smoking status. Eyes were included that had a baseline CST of 290 μm or greater and a baseline gradable diabetic retinopathy severity score (DRSS).
Ultimately, 832 eyes from the 2 studies satisfied the inclusion criteria. For the analysis based on the DRSS, 113 eyes with nongradable scores at baseline were excluded.
The results showed that the rate of DME resolution was 2.5-fold greater in patients randomized to IAI.
“The median time to first resolution was 33.0 (95% confidence interval, 28.1-40.0) weeks versus not achieved with laser treatment,” Singh said.
Regarding the baseline characteristics that may drive the time to resolution, the data, he noted, pointed to a range of such features. The multivariate analysis showed that in the patients treated with IAI, increasing CST and better BCVA were associated with a longer time to DME resolution. The hemoglobin A1c and DRSS were not significant factors.
When the investigators analyzed the tertiles of the baseline BCVA, they found that “in the IAI-treated group the highest tertile of baseline BCVA (over 66 letters) was associated with a 20% lower rate of DME resolution versus the lowest tertile (57 letters or less). Similarly, the highest baseline BVCA tertile was associated with longer median time to first DME resolution versus the lowest tertile (44.1 vs. 28.4 weeks).”
Another finding was that thicker baseline CST was associated with a longer time to DME resolution. The investigators reported, “In the IAI group, the tertiles of increasing CST were associated with a significantly longer median time to DME resolution (20.1, 39.1, and 49.1 weeks for tertiles 1, 2, and 3 respectively) and lower cumulative incidence of the event (hazard ratio 0.6 and 0.6 for tertiles 2 and 3 vs tertile 1, respectively). The results for the laser-treated patients were similar.
“This pooled analysis of data from the VISTA and VIVID studies in patients with DME, thicker CST and better BCVA in the IAI group were baseline factors associated with longer time to and lower rate of DME resolution,” Singh concluded. “The baseline hemoglobin A1c or DRSS category did not affect the DME resolution. These findings may inform physicians and patients regarding expectations of DME therapy.”
---
Rishi P. Singh, MD
E: drrishisingh@gmail.com
This article is adapted from Singh’s presentation at the American Society of Retina Specialists 2021 annual meeting. Singh is a consultant to Regeneron Pharmaceuticals, which funded the study.
Related Content: Additional ASRS 2021 Content | Conference Coverage | Ophthalmology
Newsletter
Keep your retina practice on the forefront—subscribe for expert analysis and emerging trends in retinal disease management.
















