
PACK-CXL researchers continue to clear hurdles of topical drugs


This article was reviewed by Jose Gomes, MD, PhD
Antimicrobial resistance, epithelial toxicity resulting from frequently instilled fortified and toxic drugs, and lack of compliance with drug regimens are all problems associated with topical therapies.
These three factors cry out for a new approach to treating corneal diseases, and collagen crosslinking (CXL) may be a new strategy, according to Jose Gomes, MD, PhD, professor of ophthalmology, Cornea and External Disease Service, Paulista Medical School/Federal University of Sao Paulo, Brazil.


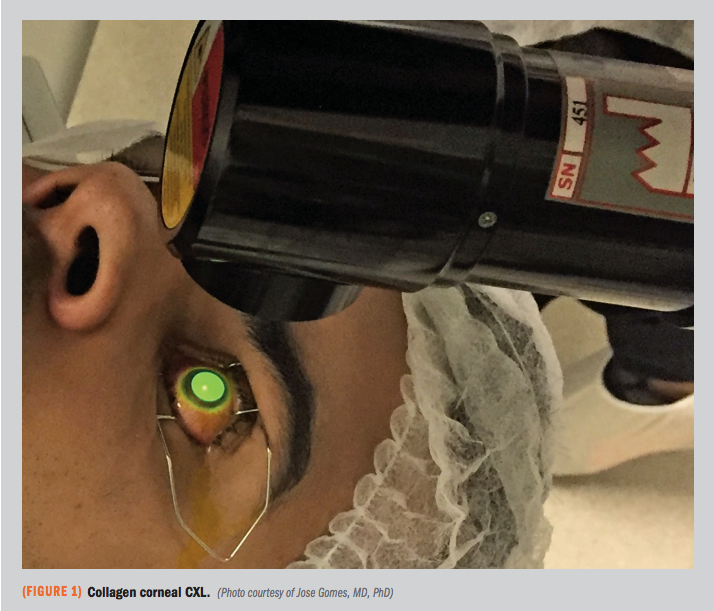
Photochemical CXL works by increasing the stiffness of the corneal tissue. Besides, CXL has the added benefit of a disinfectant effect that is achieved by combining ultraviolet A (UVA) plus riboflavin, he said.
Related: Corneal collagen crosslinking imperative in paediatric keratoconus
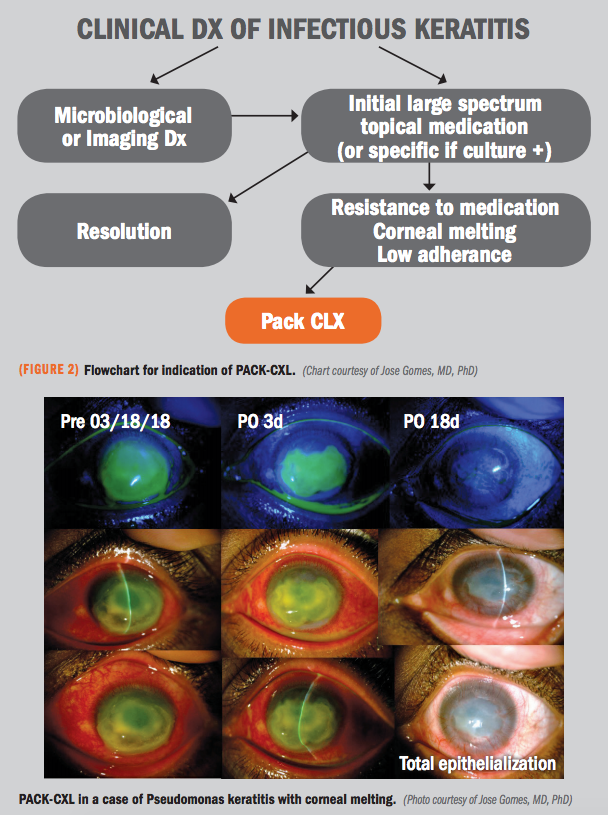
Photo-activated chromophore for keratitis (PACK) CXL may be considered the next therapeutic step in cases of confirmed infectious keratitis in which atimicrobial resistance rears its head.
The technology has been used to treat non-infectious keratitis for years, and in 2016 started to be used to treat mild cases of infectious keratitis, Dr. Gomes pointed out.
Indications, limitations
In vitro and in vivo studies and clinical case series have reported the beneficial effects of PACK-CXL for infectious keratitis.
Dr. Gomes cited a pre-clinical study of the in vitro effect of riboflavin/UVA for treating bacterial and fungal isolates that reported that some gram-positive and gram-negative bacteria but not fungi are susceptible to CXL (Martins et al. Invest Ophthalmol Vis Sci. 2008;49:3402-8).
Related: CXL imperative in treatment of pediatric keratoconus
However, previous treatment with amphotericin B allowed riboflavin/UVA effectiveness against Candida, Fusarium, and Aspergillus (Sauer et al. Invest Ophthalmol Vis Sci. 2010;51:3950-3953). The in vivo results of PACK-CXL also showed beneficial results in an animal model of fungal keratitis (Ãzdemir et al. Acta Ophthalmol. 2019;97:e91-e96).
In clinical studies, case series have reported that CXL helps in managing advanced microbial keratitis refractory to topical medical therapy (Shetty et al. Br J Ophthalmol. 2014;98:1033-5).
A combination of medical therapy and CXL or CXL alone can be efficacious, Dr. Gomes said. He also described a case of Pseudomonas keratitis treated with PACK-CXL at the Paulista Medical School, Sao Paulo. The case resolved well by day 18 after treatment with CXL.
CXL also was shown to reduce the time to resolution of suppurative fungal corneal ulcers, as reported recently (Basaiawmoit et al. Cornea. 2018;37:1376-8).
“We in Brazil also found that some cases of fusarium keratitis responded well to CXL, especially when the fungal infection was more superficial in the corneal tissue,” Dr. Gomes said.
Related: Doing justice to corneal irregularities
Study of infectious keratitis
Another study of 40 cases with infectious keratitis showed that PACK-CXL was effective when the depth of the infection was shallow, and the success rate was higher for bacterial infections compared with fungal infections.
An important finding was that riboflavin/UVA should not be applied in eyes with a previous herpes simplex infection. (Price et al. J Refract Surg. 2012;28:706-13).
Acanthamoeba may be the pathogenic exception to the response to CXL. The in vitro results did not show a good response to Acanthamoeba trophozoites or cysts.
This finding also was true for the in vivo model of infection. However, in the clinical setting, a few reported cases had contradictory results. In 2011, Khan et al. (Ophthalmology. 2011;118:324-331) described the resolution of three cases of acanthamoeba infection following CXL.
Related: Estimating the total corneal power key in keratoconus patients
In a multicenter, prospective, comparative study including eyes with infectious keratitis and corneal melting treated with PACK-CXL and antimicrobial therapy (21 eyes) or only antimicrobial therapy (19 eyes), Said et al. (Ophthalmology. 2014;121:1377-82) found a complication rate of 21% in the control group, whereas there was no incidence of corneal perforation or recurrence of the infection in the PACK-CXL group.
These results indicate that PACK-CXL may be an effective adjuvant therapy in the management of severe infectious keratitis associated with corneal melting.
A few meta-analyses are evaluating the efficacy of PACK-CXL. One of them that included 12 reports with a total of 104 eyes treated with CXL showed the same results as found previously and corroborated the results with bacterial infections and acanthamoeba cases more so than with fungal keratitis (Papaioannou et al. Cornea. 2016;35:62-71).
Related: Hardware, software offer surgeons a window to cornea diagnosis
New perspectives
The period of 2018 to 2019 saw the introduction of accelerated CXL. As seen previously, cases of bacterial keratitis fared well. A new device (C-Eye Technology, EMAGine) that can be mounted onto the slit lamp is available and facilitates more focused treatment.
Rose Bengal plus 518-nanometer green light (rose Bengal photodynamic antimicrobial therapy) is another new wrinkle in CXL. With this technology, fungal and bacterial keratitis both responded well to CXL and more so than riboflavin (Amescua et al. Cornea. 2017;36:1141-1144).
Related: Traversing the CXL pathway: Where do we go from here?
Dr. Gomes reported that researchers at the Paulista Medical School are conducting in vitro studies using PACK-CXL with 0.1% rose Bengal under green light-emitting diode irradiation and found complete growth inhibition of Staphylococcus, Pseudomonas, and Mycobacterium.
When the technology was applied to clinical cases, the researchers achieved better results with fungal keratitis than the results previously achieved with riboflavin.
Dr. Gomes concluded that these studies have shown that CXL can be considered an adjunct treatment for infectious keratitis, especially in cases that have been refractory to conventional therapy.
“CXL is effective for both bacterial and some cases of more superficial fungal and acanthamoeba keratitis,” he said. “Fast CXL and new photoactivated chromophores such as rose Bengal can improve the results by making the procedure faster and safer.”
Read more by Lynda Charters
Jose Gomes, MD, PhD
E: japgomes13@gmail.com
Dr. Gomes is a consultant to Alcon, Allergan, Bausch + Lomb, Mundipharma, and Ofta Vision Health.
Newsletter
Keep your retina practice on the forefront—subscribe for expert analysis and emerging trends in retinal disease management.











